Vital Points
Shot placement, incapacitation and conventional wisdom

Gail shooting the Walther PPQ .45 ACP.
Many, if not most, defensive firearms programs these days emphasize three points of aim on deadly human opponents: center chest, brain and pelvic girdle. However, the last one, the pelvic girdle, has come under fire from some quarters as not being effective. This is worthy of debate.
Jim Cirillo was a good friend of mine from the early 1970’s until his death, and I learned a great deal from him, his partner Bill Allard, and other members of the legendary NYPD Stakeout Squad. In Jim’s Guns, Bullets, and Gunfights (Paladin Press) he said, “We found that whenever we shot gunmen in the pelvis or butt, they were knocked off their feet. They could still be dangerous, but at least their aim would be disturbed.”
Obviously, an offender wielding a knife or club would be out of action at that point since—without mobility—they could no longer approach to stab or strike. And even a downed gunman would now be stabilized and much easier to hit with a (hopefully) fight-stopping brain shot if he tried to shoot from the ground. More recently, a retired SEAL with extensive combat experience told me pelvic shots worked dynamically for him and his colleagues.
Can the pelvic hit fail? Of course. A mere hairline fracture of the pelvic girdle—or just a neat, round hole drilled through it—can’t be expected to have much immediate effect. A bullet that merely chips the top off the ileac crest is about like shooting the tail fin off a 1959 Cadillac, it simply won’t break down the whole machine. But put a powerful handgun bullet close to where the pelvis joins the femur, and instant collapse is highly likely. Ditto a bullet that smashes the sacrum. Pelvic shots may not guarantee “1-shot stops,” but neither do head or center chest shots. So let’s take a look at them as well.
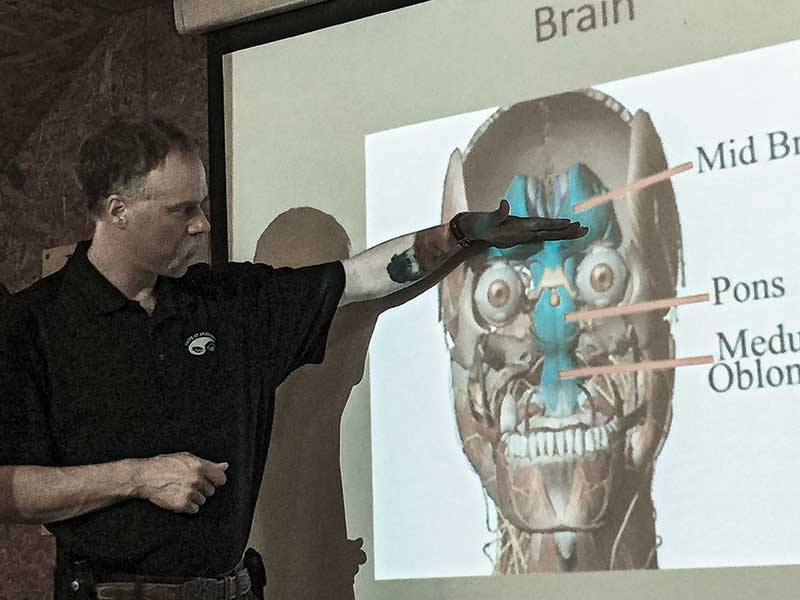
Frank DeYoung shows the part of the brain where a bullet will cause
the fastest stop during his Threat Anatomy course. Photo: Gail Pepin
Head Shot Failures
The human skull is a helmet of bone, and gunfight literature is replete with cases of bullets ricocheting off them as well as bullets homing toward the brain being deflected by the orbital sockets or upper or lower mandibles. “Shoot him in the face” isn’t a guaranteed stop, either.
In Jim Cirillo’s book he recounts one gunfight in which two of his colleagues armed with 2-inch .38 Specials (a 6-shot Colt and a 5-shot S&W Chief Special) emptied their guns into an armed robber’s face and neck, scoring 100 percent hits. When he fell, both officers thought it was over. They were shocked moments later when the man sat up. He had been hit all 11 times in vital areas, but none of the bullets reached his central nervous system. Fortunately the man had decided to cease hostilities by that point.
Jim Cirillo’s classic book is filled with hard-earned wisdom
on the subject of shot placement. Photo: Gail Pepin
More Examples
Jacksonville, Florida: Ambushed and severely wounded by multiple .45 rounds, including one to the face that deflected off course when the RN FMJ round hit his lower mandible, Officer Jared Reston shot the gunman seven times with his .40-caliber GLOCK 22 before the battle ended. Reston’s last three rounds of Winchester 180-grain JHP had struck the would-be cop-killer in the face, but only the last reached the brain and concluded matters.
Skokie, Illinois: In a nearly minute-long gunfight, Officer Tim Gramins shot his heavily armed opponent 17 times, the last three times in the head. Only the very last of those 230-grain .45 ACP Gold Dots from Gramins’ GLOCK 21 ended the death battle.
Both these instances demonstrate there’s a lot of “head” that isn’t “brain.”

Anatomy targets like this one include the three primary targeting zones.
Hitting them quickly while under stress isn’t easy. Photo: Gail Pepin
Chest Shot Failures
There’s a reason cops and well-trained armed citizens practice “failure drills” for when chest shots don’t take immediate effect on deadly opponents. If the brain is fully oxygenated, the heart can be blown completely out of the body and conscious, purposeful activity may continue for 15 seconds or more afterward. And not every heart shot results in cardiac shutdown.
There are countless survivors of cardiac gunshot wounds walking around as you read this. I’ll never forget talking to LAPD cop Stacy Lim, who was shot in the heart with a .357 Magnum, returned fire and killed her assailant with six rounds from her 9mm Beretta. She was back on duty in a few months and went on to become one of the great role-model police academy instructors.
We have to bear in mind that the human body is an amazingly resilient machine. Your opponent may be fueled with pain-killing alcohol or heroin, adrenalin-releasing cocaine, and assorted other drugs which—along with pure hate and rage—can keep him up and running despite massive, mortal wounds.
Attend the Threat Anatomy class from experienced and gun-wise paramedic Frank DeYoung or the Tactical Anatomy course from gun-savvy Dr. Jim Williams. Or you can at least read Williams’ Tactical Anatomy. Understand that it’s not just “head, chest, pelvis” and it’s certainly not “center of mass.”
If you think about it, “center of mass” would be halfway between the crown of the skull and the soles of the feet of a standing opponent. Thus, it’s pretty much a prescription for a gut shot. While it might be eventually fatal, there’s simply nothing there anatomically that—if caused to stop functioning by a bullet—would render an assailant incapable of pulling a trigger or lunging with a knife.
Anatomic aim is the key. Dr. Williams calls it “X-Ray Aim.” Know where the parts are that will shut down the human machine trying to kill you. Not just chest, but heart (and preferably heart into spine). Not just head, but brain (preferably deep brain to reduce the likelihood of last-moment trigger-pulling or bomb-triggering spasmodic reflexes. And yes, it can be a shot that breaks the pelvis in a place where that big circle of bone can no longer support the body.
It isn’t easy. But life or death issues never are.
Threat Anatomy LLC
www.threatanatomy.com
Tactical Anatomy
www.tacticalanatomy.com
RELATED ARTICLES

Shoot Smaller...

S&W Model 52



